At six months of age, Case 6 was a happy baby. She locked eyes with people and smiled back, reacted when her name was called, and enjoyed playing ‘peek-a-boo’. By twelve months, she babbled and knew three words. Six months later, she hadn’t learned any new words. She didn’t point at things to ask for them, as normally developing babies do at this age. She fell frequently and began hitting herself on the head. At 36 months of age, she was diagnosed with autism.
Many parents whose children have been diagnosed with autism can tell a similar story. The individual details are different, but the global progress of the disorder is the same, says Lonnie Zwaigenbaum, now co-director of the Autism Research Centre at Glenrose Rehabilitation Hospital in Edmonton, Canada, one of the leaders of the study that included Case 6. The girl labelled ‘Case 6’ was part of a study that followed, from infancy to toddlerhood, the younger siblings of children diagnosed with autism. Baby sibs, as researchers affectionately call them, are at a much higher risk of developing the disorder than the general population. One in five baby sibs will be diagnosed with autism1; the prevalence in the general population is 1 in 88.
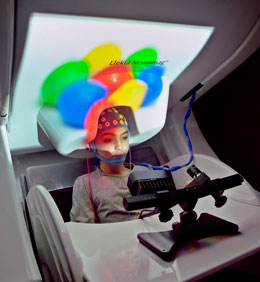
A child at low risk for autism wears an electrode cap, which captures the faint electrical signals generated by neurons, as part of a study on autism development.
Because the population of baby sibs is almost 20 times richer in children who will go on to develop autism, this cohort is ideal for studying the origins of the disorder. In baby sib studies, researchers record the behaviour, cognitive ability and brain function of baby sibs throughout development, as well as infants the same age who do not have any siblings with autism. By comparing the developmental trajectory of the two groups, they hope to gain a better understanding of how autism unfolds. But more importantly, researchers are on the hunt for markers that might enable them to identify infants at high risk of autism in the general population, while developing earlier interventions.
The story of babies like Case 6 does not have to be set in stone at birth. “There is no reason to accept the disabling consequences of autism,” says Mayada Elsabbagh, a psychiatrist at McGill University in Montreal, Canada, who studies the brain function in autism. “If we start intervention earlier, when the brain is more malleable, we can prevent these consequences.”
Early signs:
Autism can be diagnosed at three years of age. However, owing to disparities in access to healthcare, the median age at diagnosis in the United States is more than five years. By the time most children with autism come into the clinic, they already have major problems with social engagement and language, as well as other difficulties, such as repetitive behaviours.
Early intervention is important because autism can create a vicious cycle. Without the ability to draw people in and be drawn to them, a child will lose learning opportunities that shape the rapidly developing brain. But cause and effect are difficult to tease apart in autism, and problems in brain function are likely to precede social and language difficulties. As a result of this muddle, “by the time you see the end state, it’s hard to separate the core symptoms from their effects,” says Mark Johnson, who directs the Centre for Brain and Cognitive Development at Birkbeck, University of London. Prospective baby sib studies might fill in the gap.
In the mid-1990s, researchers started the first prospective studies that followed both baby sibs and children with no siblings with autism. The earliest of these studies focused on behavioural markers. In 2005, having followed a group of infants (including Case 6) from six months of age, Zwaigenbaum co-authored one of the most influential baby sib studies to date2. Based on this investigation, Zwaigenbaum says, while there is a clear global progression of behaviours in baby sibs who go on to develop the disorder, when each infant is watched individually, there are exceptions.
Eye trackers and magnetoencephalography scanners detect neural activity and are helping to quantify the early cognitive signatures of autism.
At six months, most of the babies who go on to develop autism are in line with their peers. Like Case 6, they smile when their parents smile, and when strangers smile. Most will perk up when someone says their name. However, while most babies around this age develop the strength and coordination to hold up their heads and sit independently, baby sibs who go on to develop autism often do not. “They may be floppy — some can’t hold their head up,” says Zwaigenbaum. These early motor problems are one of the best-established early indicators of the disorder, but why they occur, or whether they might cause subsequent problems, is unknown.
After six months, the development of baby sibs who go on to develop autism seems to plateau, whereas their peers become more social, more talkative, and more creative. By 12 months, the Canadian researchers found, many children who will eventually be diagnosed with autism have started to become withdrawn. They don’t cue into what other people are doing, but may be intensely interested in non-social stimuli. For example, they may stare at toys but not play with them in ways other children do. “They don’t smile as much, they don’t light up to peek-a-boo, and they show intense visual engagement with toys,” says Zwaigenbaum. “But it’s variable — you might find they are reserved but not impaired, and they may score normally on behavioural assessments.”
Children who will later be diagnosed with autism start to show more stable, recognizable signs after 18 months. “They make poor eye contact, they don’t play [normally], and they begin repetitive behaviour,” says Zwaigenbaum. At this age most normally developing children begin pretending with toys, but a child who goes on to develop autism is less likely to. Instead of playing imaginatively, the child may, for example, put the wheels of a toy car up to his or her face and stare intently as they spin.
Although these behavioural and motor signs are clearly correlated with an autism outcome, says Zwaigenbaum, neither his group of children nor any others have demonstrated that they can be used to predict the disorder. Yet even though the results are confounding, they also offer hope. Baby sibs who do not go on to develop the disorder often score as atypical at some point, compared with infants who have no siblings with autism. This suggests that for some baby sibs — who are presumably at higher genetic risk for the disease — there may be protective factors at work that researchers could identify and encourage.
Quantifying risk:
A new crop of baby sib studies goes further and deeper. Ami Klin, chief of the Marcus Autism Center in Atlanta, Georgia, is trying to fill in autism’s developmental map with dense, quantitative data on behaviour. His approach is to measure early and often. He believes this is the only way to get at the richness of normal development in the first year of life, and how it goes awry in autism. In his group’s studies, the children are assessed monthly for their first 6 months, then every 3 months until they reach 24 months of age. Measuring once every 6 months, he says, is like “sending a spaceship to another planet, taking a picture from far away, and saying, ‘no water’,” — without ever sending a rover for on-the-ground exploration.
Klin’s lab is developing technologies to quantify infant attention. One of these is an eye-tracking system that very densely samples where infants look, as often as 60 times a second, with software to analyse the data. Klin developed these tools and tested them in older children with autism. For example, Klin’s group reported3 an eye-tracking test that compared how attentive toddlers with and without autism were to social and non-social motion by tracking them while they watched simple animations. Toddlers without autism preferred to look at human motion, whereas those with autism showed no preference.
Klin has now done similar vision-tracking experiments in baby sibs, although the results haven’t been published yet. He is waiting for the children to reach 36 months, when the autism diagnosis is considered stable, so he can compare baby sibs who did and did not develop the disorder with the control group. He’s also working with speech scientist Gordon Ramsay of the Yale Child Study Center in New Haven, Connecticut, to make monthly recordings of the babies’ vocal environment, to watch how they progress from babbling to language, and how they learn to modulate their voices to convey emotion.
The chicken and the EEG:
Behavioural checklists and quantitative measures of cognition such as Zwaigenbaum’s and Klin’s may eventually lead to a test that paediatricians can use to identify high-risk babies in the general population. To complete the developmental map of the disease, other researchers are undertaking studies of brain function. But there’s still a chicken-and-egg problem in autism: do problems in brain function precede behavioural problems, or vice versa? And to what extent do these feed off one another?
“Changes in brain development precede changes in behaviour,” states Charles Nelson, director of research for the Developmental Medicine Center at Boston Children’s Hospital in Massachusetts. Nelson’s is one of a handful of groups studying brain function in baby sibs. Since most behavioural signs of autism emerge after the first year, Nelson and others believe that the key will be to find the origins of autism in the brain during the critical first 12 months of life. Early results from a handful of these studies have come out this year, and many more will follow.
One of the most powerful tools available to developmental neuroscientists such as Nelson is electroencephalography, or EEG. Researchers fit babies with electrode caps that capture faint electrical signals generated by neurons firing on the surface of the brain. In 2012, Nelson’s group showed that 6-month-old baby sibs, when resting, showed lower levels of all types of EEG activity compared with low-risk babies4. His group is still processing data from older ages.
In the spring of 2012, researchers led by Johnson and Elsabbagh showed that brain function between 6–10 months of age could be used to predict which baby sibs will be diagnosed with autism at 36 months of age5. While monitoring them with EEG, the researchers showed the babies two images: one of a woman looking at the viewer, and one with her eyes averted. Most of those who did not develop autism showed a different EEG response depending whether the woman’s gaze shifted to or away from them. Babies who were later diagnosed with autism did not appear to differentiate.
In these brain studies, as in the behavioural studies, the clearest differences were not between infants who developed autism and those who didn’t, but between high-risk infants — the baby sibs —and low-risk infants. “Most babies at risk are processing stimuli differently, but many compensate for that” and do not develop the disorder, says Johnson. Perhaps they compensate because the infant brain is plastic, or perhaps they have a particularly supportive environment. Whatever it is, it’s giving researchers hope that there might be protective effects — and that early interventions could eventually alleviate autism.
It may be a decade or more before behavioural and brain-function studies in baby sibs yield a reliable checklist that can be used to predict the risk of autism in the general population. For one thing, researchers can’t crunch the numbers until three years into the study, when the children reach an age at which a stable diagnosis of autism can be determined. And then, once the data from these prospective baby sib studies are sufficiently robust, researchers will then have to use them to test babies in the general population and follow them until 36 months as well.
In the meantime, some researchers are testing infant interventions in baby sibs even without having a reliable prediction of autism. Because only one in five of these children will receive a diagnosis, any intervention has to be supportive and positive for both the infant and the parents, regardless of whether the child develops autism. Programmes in testing emphasize fostering the relationship between parent and baby — something that’s good for any family, and that may have particular benefits for children who will go on to develop autism, perhaps lessening their eventual symptoms, says Jean Kelly, co-director of the Center on Infant Mental Health and Development at the University of Washington in Seattle.
Whether improving parent–baby relationships works to lower the risk of autism is the subject of baby sibs intervention studies at the University of Washington and elsewhere. Kelly’s group takes videos of parent–child interactions, and coaches parents — many of whom are stressed because they already have a child with autism. Kelly holds these sessions weekly for 3 months with baby sibs 8–15 months of age. Kelly’s group is trying to help teach, “How do I reach this child?” And, she says, “we are promoting trust, security and attachment on the side of the child.”
Rebecca Landa, director of the Center for Autism and Related Disorders at the Kennedy Krieger Institute in Baltimore, Maryland, has seen the power of interventions in high-risk toddlers from two years of age and is now trying to use these measures in babies. Some of the interventions her group is studying involve bringing together 12-month-old baby sibs who have shown troubling behavioural signs. The group then performs social tasks that take advantage of the peculiarities of repetitive autistic behaviours to encourage them to imitate one another — something these children normally won’t do. These children tend to move objects back and forth and stare at them, so if the researchers give them all the same object, they end up doing the same motion, and then they notice one another. In one exercise, the 1-year-olds wipe the table in front of them with wet wipes, and the researchers then get them to sing “This is the way we wash the table” and carry the wipe to the bin.
After this exercise, says Landa, “the parents are in disbelief that the children are doing an activity they normally do at home, that they’re learning the words ‘wash table’, that they are socially engaged,” she says. The intervention studies are still in progress, but Landa is optimistic. “We want to stop these problems in their tracks,” she says. If these methods are shown to have benefits for baby sibs, Landa and Kelly both hope to develop a standardized program that could be widely implemented by paediatricians and child minders.
“For some of these babies, autism doesn’t have to be their destiny,” says Johnson. Genes influence the path of development, but the course of development is not inevitable.
This article was originally published on Child development: The first steps